
min read
This article is re-posted from User Centric’s blog.
Have you ever been able to master the workings of your refrigerator/freezer temperature controls, the myriad of combination settings on your washing machine, or your new mobile phone and the set up to automatically sync with your Outlook? If not, you are certainly not alone. Products that are intuitive to use do not come to market by luck. It takes specialized knowledge and focused research to design a product that people can understand and use.
There are fields of study (e.g. human factors, cognitive psychology, anthropology) and experts who observe and measure the usability of everyday things. Some focus on how we use products such as remote controls, appliances, and doors. Others focus more directly on how humans interact with technology. The concept of researching users in their everyday environments and conducting usability studies to measure and improve how we use products and technologies has been around for quite some time. It has been embraced by industries such as communications, aviation, and medical devices. Even the fast-food industry has invested significant research into the design and usability of their point of sale systems which offer flexibility to the customer as well as increased efficiency during the ordering process. Historically, we have not seen this same amount of rigor put in to measuring HIT system usability and optimizing user interfaces.
Undoubtedly, HIT solution providers have invested significant effort into designing systems that provide a required level of security and privacy and that also provide the needed functionality to support frequent and life-critical tasks of their key users. Furthermore, significant thought has also been invested in how to best to support the user by capturing and displaying information electronically and in meaningful ways that can improve and streamline the decision-making process. Nevertheless, significant challenges still exist in designing EHR systems that are truly easy to use, intuitive, and return real value in the form of decision support, intelligence, data aggregation, meaningful display, and ultimately support improvements in patient care.
There is substantial anecdotal evidence and a growing list of peer-reviewed published research that show poor usability is a key barrier to the adoption of EHR systems. Systems that are perceived as overly time-consuming or difficult to use also have a negative impact on the quality of healthcare data entered by healthcare providers Many of you are currently using, implementing, or planning for EHRs with the goal to streamline processes and improve quality of care in your clinical practices. Given the complexity of EHR systems today, it is critical that they are easy to use to ensure safety and to enable clinicians to focus on their patients rather than on their EHR.
In instances where clinical needs call for truly different processes (e.g. different specialty needs, e.g. endocrinology- insulin sliding scale dosing, cardiology- anticoagulation clinic and Coumadin dosing), the system design and flow must provide the flexibility necessary to support those differences. As is often the case, this increased flexibility also creates the potential for usability issues. To that end, EHRs must be designed and built for flexible, efficient, and error-free use. They must return real value and support the end user’s goals. Otherwise, they are essentially data-entry systems with very little information or intelligence provided back to the user.
The good news is that with research methods already on hand, EHR usability can be measured, tracked, and improved today. Coupled with health care domain experts, human factors and user-research experts will be able to provide the critical tools, methods, and knowledge to effectively study how humans are interacting with the systems. As a team they posses more expansive knowledge to understand the combinations of user workflow and goals (operational as well as clinical) and the UI design needed to support the safest and highest quality patient care possible.
The goal of human factors research and user-centered design is to understand what users do, why they do it, how they do it, and then provide recommendations for the improvement of technology and systems to support end-user needs and goals. The use of health care IT designed in the absence of such input by the actual users may well lead to greater errors, more stress, and lower productivity. For example, a 2005 JAMA study highlighted a number of new risks for medication errors introduced when an electronic prescribing system was implemented. Many of these potential errors were the result of usability problems with the interface. In a clinical environment, these errors can have very serious or even lethal implications.
One such study showed that a widely used CPOE system facilitated 22 types of medication error risks. Examples include fragmented CPOE displays that prevent a coherent view of patients’medications, pharmacy inventory displays mistaken for dosageguidelines, ignored antibiotic renewal notices placed on papercharts rather than in the CPOE system, separation of functionsthat facilitate double dosing and incompatible orders, and inflexibleordering formats generating wrong orders (Koppel, 2005). Many of these error risks were only identified after both qualitative and quantitative research with focus groups, expert interviews, surveys and shadowing users.
Targeted human factors research can help to determine:
• High-volume, efficient workflow that should be supported by EHR systems
• Current and prospective usability issues faced by clinical team members during patient care activities
• Real-world impact of EHR systems on clinical resources and quality of healthcare data
• Trouble spots on EHR workflow and major interface issues
Examples of proven user research methods from the behavioral sciences:
• Workflow analysis and end-user interviews – to ensure accuracy of mental models
• Time and motion performance analysis – to measure efficient user performance
• Eye-tracking – to measure perception and attention
• Quality surveys – to assess end-user satisfaction and confidence
As most are aware, many EHR deployments do not always go smoothly and often times result in low adoption rates or sometimes fail altogether. There are various reasons for this, but one at the top of the list is poor user interface/application flow designs or the poor fit between design with a specific use context. It has been shown through research that clinicians demonstrate consistent patterns when navigating through the EHR to perform different clinical tasks (Zheng, 2009). Some of these patterns were unanticipated, significantly deviating from the ideal patterns according to the system’s original design principles. Better understanding the nature of this deviation can help to identify undesirable user behavior and/or design deficiencies, informing corrective actions such as more focused user training or continued system and UI redesign.
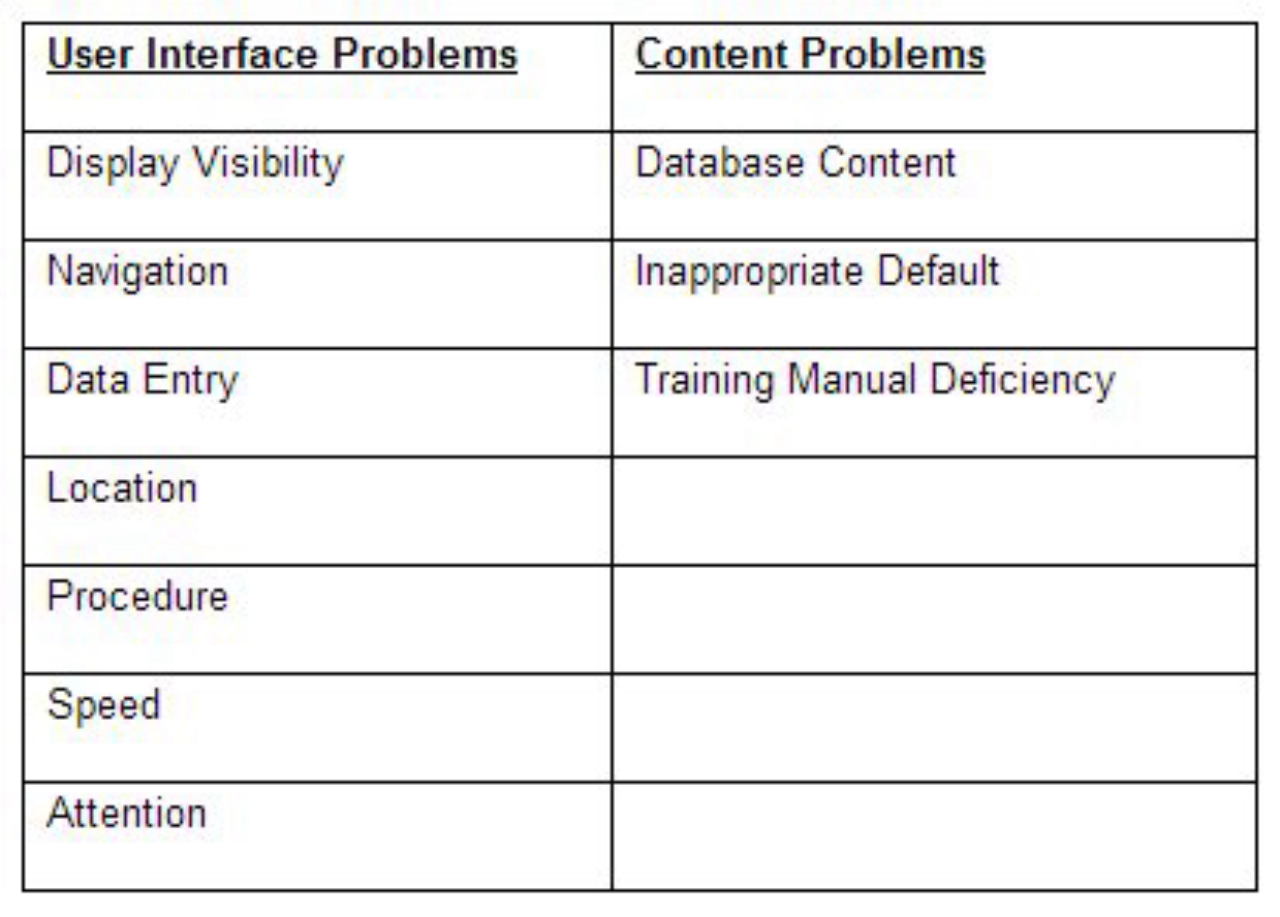
Samples of common UI and content problems
It is wise for EHR users to develop close relationships with their solution partners and continually provide feedback around usability and demand improvements if necessary. This conversation is more effective when the implications of such change are also discussed. In addition, consider inviting product managers and developers to spend time at your organization and observe the users in their daily environments and routines as this does not occur nearly as much as it should in the development lifecycle. By placing greater emphasis on and investment in usability during product design and testing, you can ensure that usability problems are addressed prior to system deployment and potential negative impact on patient care.
So, the next time you find yourself using a new technology and thinking “This was so easy to use!” – remember that there is a lot of research and effort put forth to understand how you, the consumer, will use it.
References:
Koppel, R. (2005). Role of Computerized Physician Order Entry Systems in Facilitating Medication Errors. JAMA, 293(10), 1197-1203.
Kushniruk, A. (2008). Combining Two Forms of Simulation to Predict the Potential Impact of Interface Design on Technology-induced Error in Healthcare. 17th Annual International Conference on Health Sciences Simulation (ICHSS'08). 497-504.
Zheng, K. (2009). An Interface-driven Analysis of User Interactions with an Electronic Health Records System. JAMIA, 16:228-237.